It’s not surprising to learn that there’s a lot of variation in the life prospects of North Carolina children, depending on where they live. We have known this all our lives.
Even a newcomer who takes a back road on a beach trip can see the change in economic prospects from urban center to rural town. (It’s true for the mountains, too.)
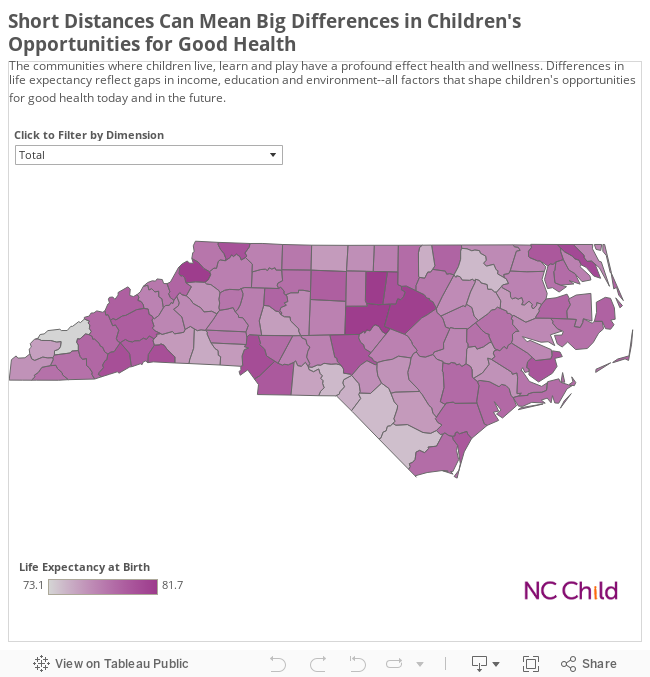
But no matter how many times you’ve heard about the plight of poor counties, our new county data cards on child health confirm the deeply troubling truth: A child’s “luck” in life—his or her chances of chronic disease or early death—is strongly correlated with factors like poverty, access to health care, and low birth weight.
The data show dramatic variations across the state, with children living in the Triangle and other large metropolitan counties enjoying better health than children in smaller, more rural communities. Drive the 53 miles between Orange and Vance Counties—and child life expectancies fall by seven years, from the state high of 81.7 to 74.8 years.
But there are also dramatic differences strictly among rural counties. The far Western counties of Transylvania and Swain, which are separated by just 80 miles, show the same gap of seven years, from the relatively richer Transylvania, to Swain, one of the smallest, poorest counties in the state. (It’s tempting to spend a couple of hours digging through every county to see where they rank.)
The good news is that we know what to do to improve the situation, and it works. It won’t solve every problem of regional economic inequity, but making some strategic policy decisions will put every county on a brighter path.
In the 20th Annual Child Health Report Card we released earlier this year, we showed how North Carolina has made good progress on increasing children’s access to health insurance, cutting the state infant mortality rate, and reducing teen pregnancy since the 1990s by investing in health care for poor pregnant women, supporting the state Children’s Health Insurance Program, and partnering with local communities to implement evidence based teen pregnancy prevention programming.
It is completely within our grasp to make significant inroads in the distressing predictions of life expectancy and chronic disease, but we have to get started now. These are the three key steps we recommend:
- Strengthen access to health insurance for women of reproductive age by expanding Medicaid to cover adults below 138 percent of the Federal Poverty Line.
- Support infant mortality prevention strategies like the Healthy Babies Bundle, a package of perinatal interventions that promote strong birth outcomes, recommended by the Child Fatality Task Force.
- Invest in early intervention services to reduce the effects of developmental delays.
County leaders from even the poorest counties can use the data and policy recommendations to target budget investments to local programs with the greatest potential for cost-avoidance—the health of children. As healthier children (who are not hungry) go to school, they show up as better learners, and that reflects better on a county’s prospects for economic development. We know what the data are telling us about the “luck” of where a child lives. Let’s do what the data have shown makes a difference, because it’s really not about luck; it’s choice and hard work. And we can do it.